Knee discomfort after running? Beware of "runner's knee"! Handle it this way within 48 hours to avoid worsening
In recent years, marathons have become popular. Running, as a low-threshold activity with many benefits, is widely loved. As the number of runners has grown, the sports injury known as "runner's knee" has become increasingly common. Many runners, while enjoying the pleasures of running, must interrupt training due to knee pain or even suffer long-term knee discomfort. "Runner's knee" not only affects athletic performance but, in severe cases, can also impact daily life.
Follow the "POLICE" principle during the acute pain phase
"Runner's knee" is not a single disease but a general term referring to various knee pain problems caused by running or other repetitive flexion-extension movements. It commonly presents as a dull pain around the knee, especially worsened when going up or down stairs, squatting, rising after prolonged sitting, or during long runs.
During the acute pain phase (usually 48–72 hours after injury), the POLICE principle should be followed.
If pain is severe or there is obvious joint swelling, prompt medical evaluation is recommended to establish a diagnosis through physical examination and imaging studies, and to exclude serious injuries such as meniscal tears to avoid delayed treatment.
“POLICE”原则
The "POLICE" principle
P: Protection. Use a knee brace or kinesiology tape to temporarily stabilize the joint and avoid movements that may worsen the injury, such as deep squats and jumping.
OL: Optimum Loading. Within the limits of pain, begin gentle activities as soon as possible, such as straight leg raises.
I: Ice. Apply ice for 15–20 minutes each time, 2–3 times daily, to effectively control swelling and pain; avoid direct skin contact with the ice pack.
C: Compression. Use an elastic bandage or support to apply moderate compression, which can reduce swelling without compromising circulation.
E: is for Elevation. Elevate the affected limb above heart level during rest to promote venous return.
Rehabilitation training during the recovery phase
After inflammation in the acute pain phase is controlled (usually 3–7 days), rehabilitation should focus on strengthening muscle strength, improving flexibility, and enhancing lower limb neuromuscular control. This is a gradual process and exercise intensity should be adjusted according to individual tolerance.
Exercise the quadriceps and muscles around the hip joint
Wall-supported static squat: Back against the wall, feet shoulder-width apart, slowly squat until the thighs are parallel to the ground (knee flexion about 90°), hold the position. Ensure the knees do not go past the toes and are aligned with the second toe direction. Start by holding 15 seconds each time, gradually extend to more than 1 minute, perform 3–5 sets daily.
Straight leg raise: Supine position, flex the non-affected side knee, raise the affected straight leg to 45°, hold for 5 seconds then slowly lower. Progressively add ankle sandbag load as tolerated.
Side-lying hip abduction: Side-lying position, maintain pelvic neutrality, abduct the upper leg about 30° and slightly extend, control the leg to slowly lower, strengthening the gluteus medius. 15 repetitions per set, 2–3 sets daily.
Thoroughly relax and stretch the tight muscle groups
Foam roller release: Side-lying position; place the foam roller under the lateral thigh and slowly roll from the hip to above the knee, pausing on tender spots for 10–15 seconds until pain decreases. Perform 1–2 times daily, avoiding excessive pain. Use the same method to release the anterior and posterior thigh.
Stretching exercises: Standing with back against a wall, assume a lunge and stretch the calf muscles by keeping the rear supporting leg straight and the front knee bent to target the gastrocnemius and soleus. Hold each stretch for 20–30 seconds, repeat 2–3 times.
Strengthen lower limb neuromuscular control
Single-leg balance training: Stand on one leg and hold for 30 seconds. To increase difficulty, progress to single-leg stance with eyes closed or on a foam pad to improve dynamic stability of the knee joint.
If rehabilitation progresses well, daily activities are pain-free and a single-leg half-squat can be held for more than 1 minute, gradual running training can be considered. Rehabilitation is a long-term process; it is recommended to follow the "10% rule" — weekly running volume should increase by no more than 10% over the previous week. Also observe three key indicators after each run:
① Immediate post-run pain does not exceed 3 out of 10 (10 being worst);
② No worsening on the morning after;
③ Does not affect normal gait.
If any indicator does not meet the standard, return to the previous stage. At the same time, continue strength training and stretching, for at least 3 months after full recovery.
Acupoint massage helps recovery
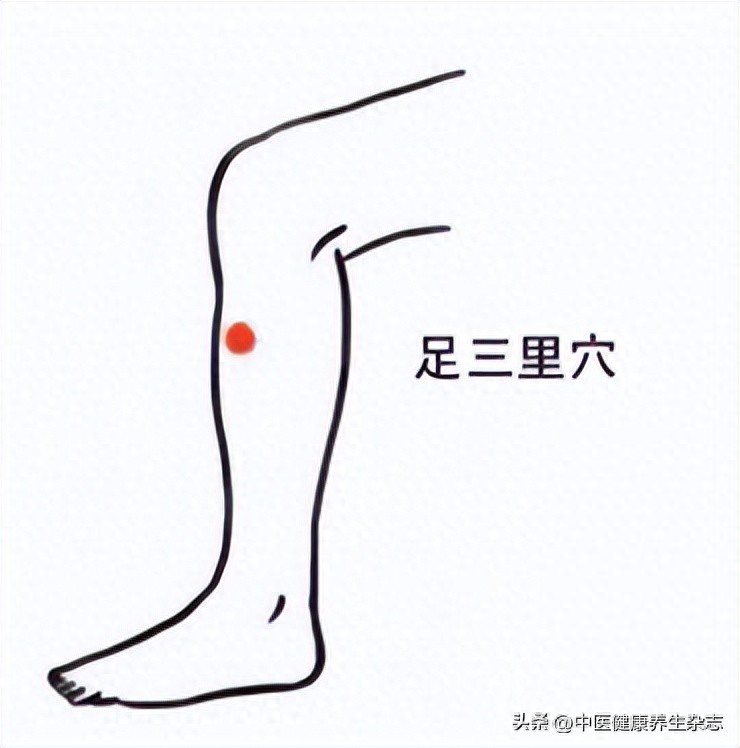
Zusanli (ST36)
Location: Lateral aspect of the lower leg, 3 cun below the lateral patellar depression (four horizontal fingers), one horizontal finger lateral to the anterior crest of the tibia.
Efficacy: Tonifies qi and blood, strengthens tendons and bones, relieves knee joint fatigue and chronic pain.
Massage method: Press firmly with the thumb and rub clockwise, 3 minutes each time.
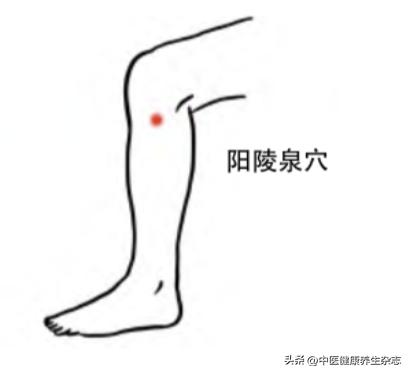
Yanglingquan (GB34) acupoint
Location: Lateral side of the lower leg, in the depression anterior and inferior to the fibular head.
Effects: Regulates liver and gallbladder, relaxes tendons and activates collaterals, improves lateral knee pain and stiffness.
Massage method: Press vertically with the thumb until a sour, distending sensation is felt; 2–3 minutes each time.
Blood Sea (Xuehai) acupuncture point
Location: Medial side of the thigh, 2 cun above the superior medial border of the patella (about three horizontal fingers), at the bulge of the vastus medialis.
Effect: Invigorates blood and resolves stasis, relieves pain and swelling of the medial knee joint.
Massage method: Rub in circular motions with the heel of the hand, 3 minutes each time.

Liangqiu (ST34)
Location: Knee flexed, anterolateral aspect of the thigh, 2 cun above the superolateral border of the patella (approximately three finger-widths).
Effect: Relieves acute knee joint pain.
Massage method: Press firmly with the thumb and rub toward the knee, 2–3 minutes each time.

Weizhong (BL40) acupuncture point
Location: At the midpoint of the popliteal crease, between the biceps femoris tendon and the semitendinosus tendon.
Efficacy: Unblocks the channels and relieves pain; alleviates posterior knee pain and muscle tension.
Massage method: Requires assistance from another person; press firmly with the thumb and gently knead with moderate force, 2 minutes each time.

Knee Yang Gate acupuncture point (Xiyangguan)
Location: Lateral side of the knee, 3 cun above the Yanglingquan (GB34) point (about four horizontal fingers), in the depression superior-lateral to the lateral epicondyle of the femur.
Effect: Relieves lateral knee joint pain and restricted movement.
Massage method: Press firmly with the thumb until a sour, distending sensation is felt, combined with knee flexion and extension, 2 minutes each time.

Note that when massaging, stop when you feel aching and distension and avoid forceful pressing; if the knee is in an acute phase with redness, swelling, heat, and pain, apply cold compresses first to reduce swelling, then switch to heat and gentle massage after 48 hours; simultaneously, perform quadriceps stretching (wall sit) and use a foam roller to relax the iliotibial band on the lateral thigh, reduce running volume, switch to running shoes with good cushioning, and correct running form errors such as excessive internal rotation; if pain persists for more than 2 weeks or worsens significantly, seek medical evaluation promptly to rule out ligament injury or meniscal tear.